
Abstract
The use of information and communication technologies is increasing in health care, and patient information is being transferred into electronic format. The aim of this study was to test the ergonomics and usability of a mobile workstation prototype in actual work situations. The mobile workstation was tested by physicians (n=5) and nurses (n=3) during and after hospital rounds. The study produced 19 requirements for a usable product. The participants rated wheel function, screen height, the mobility of the terminal, and the adjustability of the terminal height as the best usability features of the prototype. The keyboard level, the mouse level, and the difficulty to install the computer into the terminal were reported as the most important points in need of improvement. The results of this study show that having physicians and nurses make subjective judgments about the usability of a mobile workstation adds value to its design.
Practitioner’s Take Away
The results of this study suggest the following:
- Usability tests can be carried out with doctors and nurses in real hospital situations.
- SUS and VAS can be used quickly by end users when assessing the usability of a product.
- Subjective judgments made by end users in the work setting add value to the judgments of experts, even when ergonomic factors are involved.
Introduction
Physicians and nurses are highly mobile in their daily hospital routine, moving frequently between wards, outpatient clinics, diagnostic and therapeutic departments, conference rooms, and operating theaters (Ammenwerth, Buchauer, Bludau, & Haux, 2000). Health care professionals need to request and enter information at different locations, for example, on their daily ward round (Reuss, Menozzi, Büchi, Koller, & Krueger, 2004). Thus mobile technology is becoming more important in modern health care. Mobile information and communication systems in clinical routine have the potential to greatly improve communication, facilitate information access, eliminate double documentation, and increase the quality of patient care in the long run when an appropriate infrastructure is available (Ammenwerth et al., 2000; Buchauer, Werner, & Haux, 1998).
The utilization of mobile technology increases treatment and diagnostic capabilities, but it also increases the complexity of health care (Liljegren, 2006). Mobile devices may play an important role in convincing health care staff to use and handle the volume and complexity of clinical data by simplifying the integration of mobile devices into existing medical information systems (Karahoca, Bayraktar, Tatoglu, & Karahoca, 2010). However, physicians have clear access preferences when they interact with patient records during their daily rounds (Reuss et al., 2004). Increasingly health care policy and decision makers are demanding evidence to justify investments in health information systems (Kushniruk & Patel, 2004).
Various types of mobile devices are in use in health care. Personal digital assistants (PDAs), tablet PCs, and laptops installed on mobile workstations are the devices most commonly mentioned in the studies. Each of these devices clearly has strengths and weaknesses, which should be taken into account when a decision is made about the method appropriate for helping physicians and nurses interact with a number of electrical information systems during daily routines. User preferences for these kinds of devices and the situations under which different devices would be used have been studied in several papers (Andersen Lindgaard, Prgomet, Creswick, & Westbrook, 2009).
Some studies have commented about the usability of mobile workstations, but even then the focus was either on the information systems used by the mobile devices, the usability of the user interfaces of the system, or the physical properties of the computers per se (Andersen et al., 2009). However, a need for mobile workstations with better usability and ergonomics for health care workers was reported in these same studies. The studies addressed questions about the size of workstations, the ease of operation, and the mobility of the workstation (Junglas, Abraham, & Ives, 2009), each of which is an important design factor that affects the usability and ergonomics of a product.
In this paper we have used the terms usability and ergonomics side by side. According to Pheasant (1996), the objective of ergonomics is to achieve the best possible match between a product and its users in the context of the work task to be performed. On the other hand, the SFS-EN ISO 9241-11 (1998) standard states that usability is the extent to which a product can be used by specified users to achieve specified goals with effectiveness, efficiency, and satisfaction in a specified context of use. Generally speaking, considering both usability and ergonomics during the development of a medical device, and when medical technology is purchased at hospitals, is considered to be increasingly important (Liljegren & Osvalder, 2004; Martin, Norris, Murphy, & Crowe, 2008).
The aim of this study was to test the ergonomics and usability of a mobile workstation prototype in real work situations. As this study was conducted as a part of a product development process, an additional objective was to determine the most important ergonomic design factors that need to be taken into account in the final and future mobile workstation version. In this study neither the usability of the computer user interface nor the usability of the electronic patient information system was included. To be able to fully utilize a mobile workstation in a hospital environment requires that both the work processes and the Information and Communication Technology (ICT) infrastructure have been adapted for this new medical practice. In this study we wanted to investigate the use of the mobile workstation in normal work situations and to collect user experience on the new mobile workstation model, not the new way of working as such. Thus we selected users who already had some experience with mobile workstations.
Materials and Methods
The following sections discuss the mobile workstation features, the procedure used in this study, and the expert and participant evaluations of the workstation.
The Tested Mobile Workstation Prototype
The mobile workstation prototype was called SPARKe 54.1, as named by the prototype design company—Spark Ergonomics Oy Ltd (see Figure 1). The workstation could be equipped with either a laptop or a desktop computer. A laptop computer could be installed under the lockable cover case and operated by an external keyboard and a mouse, or it could be laid on the cover. For the external keyboard, there was a separate keyboard tray with a slide-out mouse tray and mouse cubby (on the right side of the keyboard tray). The mouse tray on the cover of the cart could be pulled out to the left or right of the cover. During the study only laptop computers were used, and they were operated in both possible installation settings. Additional accessories installed on the prototype were a storage basket and a rack for an additional battery.

Figure 1. Features of the tested mobile workstation: 1 – foot pedal for adjusting height, 2 – storage basket, 3 – rack for an additional battery, 4 – keyboard tray, 5 – case for the computer, 6 – lockable cover for the case, 7 – higher mouse tray, 8 – combined mouse tray and mouse cubby (lower mouse tray), 9 – lockable wheels (in front of the cart)
Procedure
This usability study was part of a product development process in which the expert evaluation and the user study data were given to the company that developed the mobile workstation prototype. Figure 2 illustrates the iterative design process. For the first phase of the study, experts evaluated a mobile workstation prototype and provided feedback. The experts’ feedback was integrated into the design of a redesigned mobile workstation prototype. The redesigned prototype was tested during the second phase of the study, the user study phase. Participants in the user study used the redesigned workstation prototype during one day in actual work situations in a hospital.
The outcome of both the expert review and the user study was a list of requirements for a usable, ergonomically designed mobile workstation. These requirements and feedback then were given to the company that designed the mobile workstation.
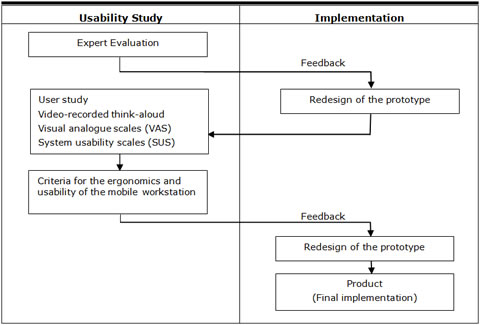
Figure 2. Procedure used during the prototype usability study. The implementation was performed by the prototype design company
Expert Evaluation
The process started with a 3-hour expert evaluation (Hignett, 1998) in which four experts in both ergonomics and technical, design, health science, and physiotherapy participated. In this hands-on session, the experts performed usage scenarios using the original prototype and commented on its physical design characteristics and the operation of the prototype. One of the experts acted as the chairman and led the discussion if needed. During the session, the experts were able to evaluate the use of the mobile workstation in simulated work situations. A laptop was placed on the prototype, but no hospital information system was available because the focus was strictly on the physical aspects of the mobile workstation.
The experts’ comments were collected during the session as a list of recommended modifications. The mobile workstation developers then redesigned the prototype with the experts’ recommendations in mind. The recommendations also served as a basis for the questions raised in the user study phase.
User Study
The following sections discuss the participants and the methods used in the user evaluation portion of the study.
Participants
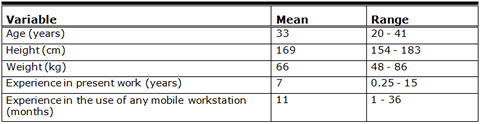
The intended users of a mobile workstation are both nurses and physicians. The practice of who operates the workstation during a round varies from ward to ward. In our study the participants were five physicians (two men, three women) and three nurses (one man, two women), aged 20-41 years (Table 1), from two hospitals in the Helsinki region of Finland. They all were right-handed and were accustomed to using a mobile workstation in their normal routine. They worked an average of 8 hours a week with their wards workstation. The volunteer participants gave their written consent to participate before the study began.
Table 1. Background Factors of the Participants (N=8), Mean and Range
Methods
The mobile workstation was tested during and after a hospital round in a hospital ward (Figure 3). A round consists of seeing all of the patients who are in the hospital under the care of the physician who leads the round. There were two rounds in this study, and the number of patients seen during rounds was between 15 and 20. One physician made the round individually; other rounds had three participants (two physicians, one nurse). The activities performed included reading the patient’s information on the screen and entering text about the patient’s status using the keyboard. After the round, the video-recorded, think-aloud method was used to further evaluate the usability of the mobile workstation prototype. The participants were asked to report their thoughts as they used the prototype. We asked the following question to all participants: "How should this product be developed further?"
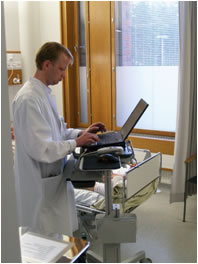
Figure 3. A physician using a mobile workstation during a typical morning round.
Visual analogue scales (VAS) were used to determine the usability features of the mobile workstation (Beauchamp, 1999; Lintula & Nevala, 2006; Nevala & Tamminen-Peter, 2004; Price, McGrath, Rafii, & Buckingham, 1983). The VAS is a 100 mm long continuous line with endpoints anchored by 0 (very poor) and 100 (very good). The VAS score is a measured distance (expressed in millimeters) from the 0 scale point. The participants were asked to mark on the line the point that indicated their evaluation of the feature. In addition, there was a question that asked, “How would you like to see this mobile workstation be further developed?”
The 10-item System Usability Scale (SUS) was used to determine the subjective assessment of the usability of the prototype (Brooke, 1996). It provided an easy-to-understand score from 0 (negative) to 100 (positive). The SUS is an effective, reliable, and inexpensive tool for measuring the usability of a wide variety of products and services (Bangor, Kortum, & Miller, 2008; Bangor, Kortum, & Miller, 2009; Dumas, 2003; Sauro, 2011).
Results
The following sections discuss the results of the expert evaluation and the user study, and the list of criteria for optimal mobile workstation design.
Expert Evaluation
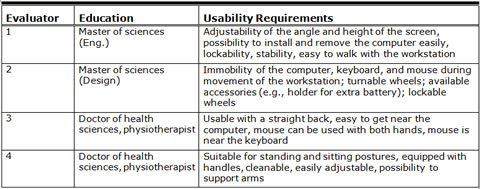
According to the group of experts, the functioning of the wheels, the height of the screen, the mobility of the workstation, and the adjustability of the workstation height were the best features of the prototype. The keyboard tray, the mouse tray, and the difficulty of installing the laptop computer onto the workstation were reported as needing further development. The evaluation showed that the design needed to be simplified (i.e., the height needed to be easier to adjust, and the case for the computer needed to be redesigned). Table 2 lists the usability requirements for any mobile workstation according to the experts.
Table 2. Expert Evaluators’ Usability Requirements for Mobile Workstations
Before the user study, the mechanism to adjust the height of the workstation and the locking mechanism of the laptop were redesigned.
User Study
This section reports the quantitative and subjective responses of the eight test participants after using the workstation for rounds. The usability of the mobile workstation according to the mean SUS index was 73 (SD 11.0). The SUS scores of the eight participants were the following: 90, 82.5 (n=2), 75, 72.5, 65, 62.5, and 52.5. There was no difference between the scores for the nurses and physicians.
The results of the VAS ratings are presented in Figure 4. Movability, the functioning of the wheels, the adjustability of the height, and the stability of the mobile workstation were the highest rated factors. On the other hand, the combined keyboard and mouse tray feature (see Figure 1) received the lowest scores. Some of the VAS ratings were heavily influenced by the work practices that individual nurses and physicians had adopted in their ward and, therefore, the ratings showed large variations. For example, some participants preferred the disinfection bottle holder on the mobile workstation as was the case in their ward, while others thought a bottle located by the patient’s bed was enough.
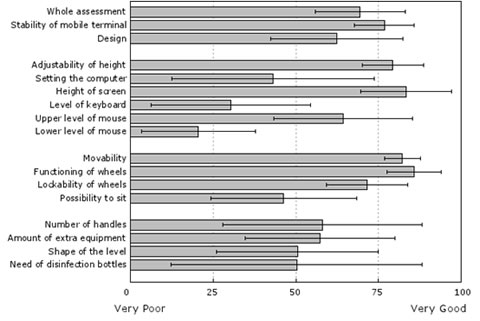
Figure 4. Perceived usability (VAS: 0=Very Poor, 100=Very Good) of the mobile workstation according to the doctors and nurses (n=8; means, standard deviations)
In response to questions, the participants pointed out that the mobile workstation must be an easy-to-use and sought-after tool for work, so that everyone would be able to make use of it easily and effectively. The doctors and nurses stated that they would like to use the mobile workstation because
"The use of the COW [computer on wheels; mobile workstation] seems very convenient."
"It is nice to make the round alone—I talk more with the patient."
"I send the instructions for the nurses and physiotherapists directly to their electronic work list."
"I have my own schedule."
All the participants were eager to comment on the usability of the new mobile workstation model because previous mobile workstation models had shortcomings. Large variations in specific VAS features clearly indicated that the basic workstation should have as simple a construction as possible, but be equipped according to users’ varying needs.
Criteria for the Ergonomics and Usability of the Mobile Workstation
Based on the findings of both the expert evaluation and the user study, we formulated the following criteria for a usable and ergonomically designed mobile workstation. These same criteria were taken as essential design points by the developers of the mobile workstation prototype.
- Small as possible
- Usable for a mobile computer, separate keyboard, and mouse
- Computer easily installed and removed
- Lockable computer or laptop
- Equipped with handles
- Computer, keyboard, and mouse stay immobile during workstation movement
- Easily moved and equipped with wheels that turn and lock
- Cleanable—no sharp corners
- Extra equipment available if needed
- Can be used when standing or sitting
- Easy to get near the computer and stand with a straight back
- Easy to adjust the height with one hand
- Height adjustability between 80-120 cm
- Angle of the screen adjustable
- Mouse usable with both hands near the keyboard
- Arms supportable during computer use
- Easy to walk with the mobile workstation, i.e., the construction of the mobile workstation does not interfere with movements of legs
- Easy to learn how to use
- Manual includes ergonomic instructions
In addition to data gathered from the expert evaluation and user study, the ErgoSHAPE method (Launis & Lehtelä, 1992) was used to define the minimum range of adjustability for the height to make it possible to work with the mobile workstation while either sitting or standing. (ErgoSHAPE is a collection of human anthropometric models and ergonomic recommendations for work place designers to be used with AutoCAD.) The recommended and minimum ranges for the height adjustment for the mobile workstation are presented in Figure 5. A range of 80–120 cm enabled even the shortest and the tallest workers (P5 or 5% of the population is shorter than 80 cm / P95 or 5% of the population is taller than 120 cm) to work comfortably with the mobile workstation, either while sitting on, for example, a saddle chair or while standing.
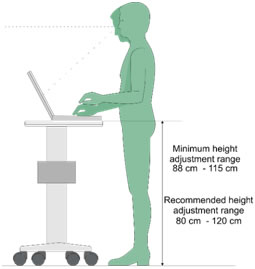
Figure 5. The recommended and minimum ranges for the height adjustability of the mobile workstation
Discussion and Recommendation
Based on the expert evaluation and the user study, this study found 19 different criteria for the ergonomics and usability of a mobile workstation. The most important ergonomic features of the mobile workstation that needed improvement were the keyboard tray, the mouse tray, and the procedure to install and lock the laptop computer to the workstation.
In the future, more information and communication technologies will be used in health care. As the market becomes more competitive, usability can be a key product differentiator and a crucial factor in the purchase decision. The results showed that a mobile workstation must be an easy-to-use and sought-after tool for work so that everyone is able to make use of it easily and effectively. Nurses and physicians need both hands for the examination and care of their patients, therefore, handheld computers are not practical. However, in the literature, no articles were found concerning the ergonomics and usability of mobile workstations: Most of the scientific literature pertained to information access in health care (Reuss et al., 2004), mobile health care acceptance (Wu et al., 2007), handheld computers (Lapinsky, 2007), and information technologies in patients’ homes (Kaufman et al., 2003).
This study was planned in cooperation with researchers, manufacturers, and experienced health care workers. As a result, it was possible to identify the work tasks generally performed with a mobile workstation and to choose proper testing methods. The final mobile workstation was developed using an iterative process that included expert evaluation and practical user experience feedback and evaluation. In the expert evaluation, four experts in ergonomics participated. The expert evaluation is a quick and cheap method for achieving broad coverage of a whole product, but it typically misses some complex issues (Barrington, 2007). In the user study, eight experienced physicians and nurses participated. It is known that the use of four to eight participants can drive a useful iterative cycle: find serious problems, correct them, and find more serious problems (Molich, 2010). According to Molich’s paper, the number and the quality of evaluators affects the results more than the size of the participant group.
This study shows that the SUS index is suitable for products other than software user interfaces. The SUS index was free, and easy to administer and use. In addition, the SUS scores can be evaluated against emerging benchmarks (Bangor et al., 2008; Bangor et al., 2009; Sauro, 2011).
References
- Ammenwerth, E., Buchauer, A., Bludau, B., & Haux, R. (2000). Mobile information and communication tools in the hospital. International Journal of Medical Informatics, 57(1), 21-40.
- Andersen, P., Lindgaard, A., Prgomet, M., Creswick, N., & Westbrook, J. (2009). Mobile and fixed computer use by doctors and nurses on hospital wards: Multi-method study on the relationships between clinician role, clinical task, and device choice. Journal of Medical Internet Research, 11(3), e32.
- Bangor, A., Kortum, P., & Miller, J. (2008). An empirical evaluation of the system usability scale. International Journal of Human-Computer Interaction, 24(6), 574-594.
- Bangor, A., Kortun, P., & Miller, J. (2009). Determining what individual SUS scores mean: Adding an adjective rating scale. Journal of Usability Studies, 4(3), 114-123.
- Barrington, S. (2007). Usability in the lab: Techniques for creating usable products. Journal of the Association for Laboratory Automation, 12(1), 6-11.
- Beauchamp, Y. (1999). Application of visual analog scales (VAS) for the comparative evaluation of tool and equipment designs and work methods. Computers & Industrial Engineering, 37(1-2), 289-292.
- Brooke, J. (1996). SUS: A “quick and dirty” usability scale. In P. W. Jordan, B. Thomas, I. L. McClelland & B. Weerdmeester (Eds.), Usability evaluation in industry (pp. 189-194). London: Taylor & Francis.
- Buchauer, A., Werner, R., & Haux, R. (1998). Cooperative problem solving with personal mobile information tools in hospitals. Methods of Information in Medicine, 37(1), 8-15.
- Dumas, J. S. (2003). User-based evaluations. In J. A. Jacko & A. Sears (Eds.), The human- computer interaction handbook: Fundamentals, evolving technologies and emerging applications (p. 1093–117). New Jersey: Lawrence Erlbaum Associates.
- Hignett, S. (1998). Ergonomic evaluation of electric mobile hoists. The British Journal of Occupational Therapy, 61(8), 509-516.
- Junglas, I., Abraham, C., & Ives, B. (2009). Mobile technology at the frontlines of patient care: Understanding fit and human drives in utilization decisions and performance. Decision Support Systems, 46(3), 634-647.
- Karahoca, A., Bayraktar, E., Tatoglu, E., & Karahoca, D. (2010). Information system design for a hospital emergency department: A usability analysis of software prototypes. Journal of Biomedical Informatics, 43(2), 224-232.
- Kaufman, D. R., Patel, V. L., Hilliman, C., Morin, P. C., Pevzner, J., Weinstock, R. S., Goland, R., Shea, S., & Starren, J. (2003). Usability in the real world: Assessing medical information technologies in patients’ homes. Journal of Biomedical Informatics, 36(1-2), 45-60.
- Kushniruk, A. W., & Patel, V.L. (2004). Cognitive and usability engineering methods for the evaluation of clinical information systems. Journal of Biomedical Informatics, 37(1), 56-76.
- Lapinsky, S. E. (2007). Mobile computing in critical care. Journal of Critical Care, 22(1), 41-44.
- Launis, M., & Lehtelä, J. (1992). ergoSHAPE – A design oriented ergonomic tool for AutoCAD. In M. Mattila & W. Karwowski (Eds.), Computer applications in ergonomics, occupational safety and health (pp. 121-128). Amsterdam, Holland: Elsevier Science BV.
- Liljegren, E. (2006). Usability in a medical technology context assessment of methods for usability evaluation of medical equipment. International Journal of Industrial Ergonomics, 36, 345-352.
- Liljegren, E., & Osvalder, A. (2004). Cognitive engineering methods as usability evaluation tools for medical equipment. International Journal of Industrial Ergonomics, 34(1), 49-62.
- Lintula, M., & Nevala, N. (2006). Ergonomics and the usability of mechanical single-channel liquid dosage pipettes. International Journal of Industrial Ergonomics, 36(3), 257-263.
- Martin, J. L., Norris, B. J., Murphy, E., & Crowe, J.A. (2008). Medical device development: The challenge for ergonomics. Applied Ergonomics, 39(3), 271-283.
- Molich, R. (2010). A commentary of "how to specify the participant group size for usability studies: A practitioner’s guide" by Macefield. Journal of Usability Studies, 5(3), 124-128.
- Nevala, N., & Tamminen-Peter, L. (2004). Ergonomics and usability of an electrically adjustable shower trolley. International Journal of Industrial Ergonomics, 34(2), 131-138.
- Pheasant, S. (1996). Bodyspace: Anthropometry, ergonomics and the design of the work (2nd ed.). London: Taylor & Francis.
- Price, D. D., McGrath, P. A., Rafii, A., & Buckingham, B. (1983). The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain, 17(1), 45-56.
- Reuss, E., Menozzi, M., Büchi, M., Koller, J., & Krueger, H. (2004). Information access at the point of care: What can we learn for designing a mobile CPR system?. International Journal of Medical Informatics, 73(3), 363-369.
- Sauro, J. (2011). A practical guide to the system usability scale: Background, benchmarks & best practices. North Charleston, South Carolina: Booksurge LLC.
- Wu, J., Wang, S., & Lin, L. (2007). Mobile computing acceptance factors in the healthcare industry: A structural equation model. International Journal of Medical Informatics, 76(1), 66-77.